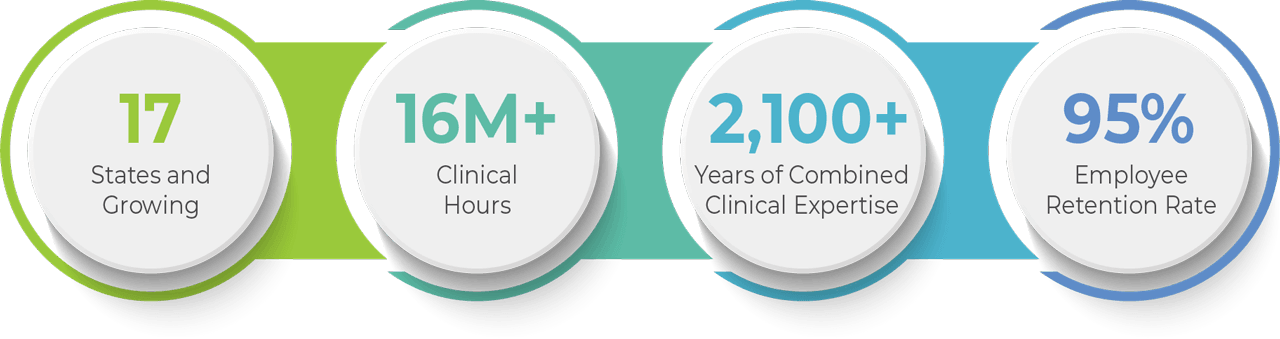
At Continuum Behavioral Health, our mission is to collaborate towards discovering the best way to ensure each individual’s right to meaningful participation within their community, and most of all, to assist every learner in reaching their highest potential.
Our Core Values
Collaboration
Do great things and learn more together
Leadership
Have the courage to shape a better future
Passion
Committed to clinical practice and education
Best Practice
Providing science-based and data-driven interventions
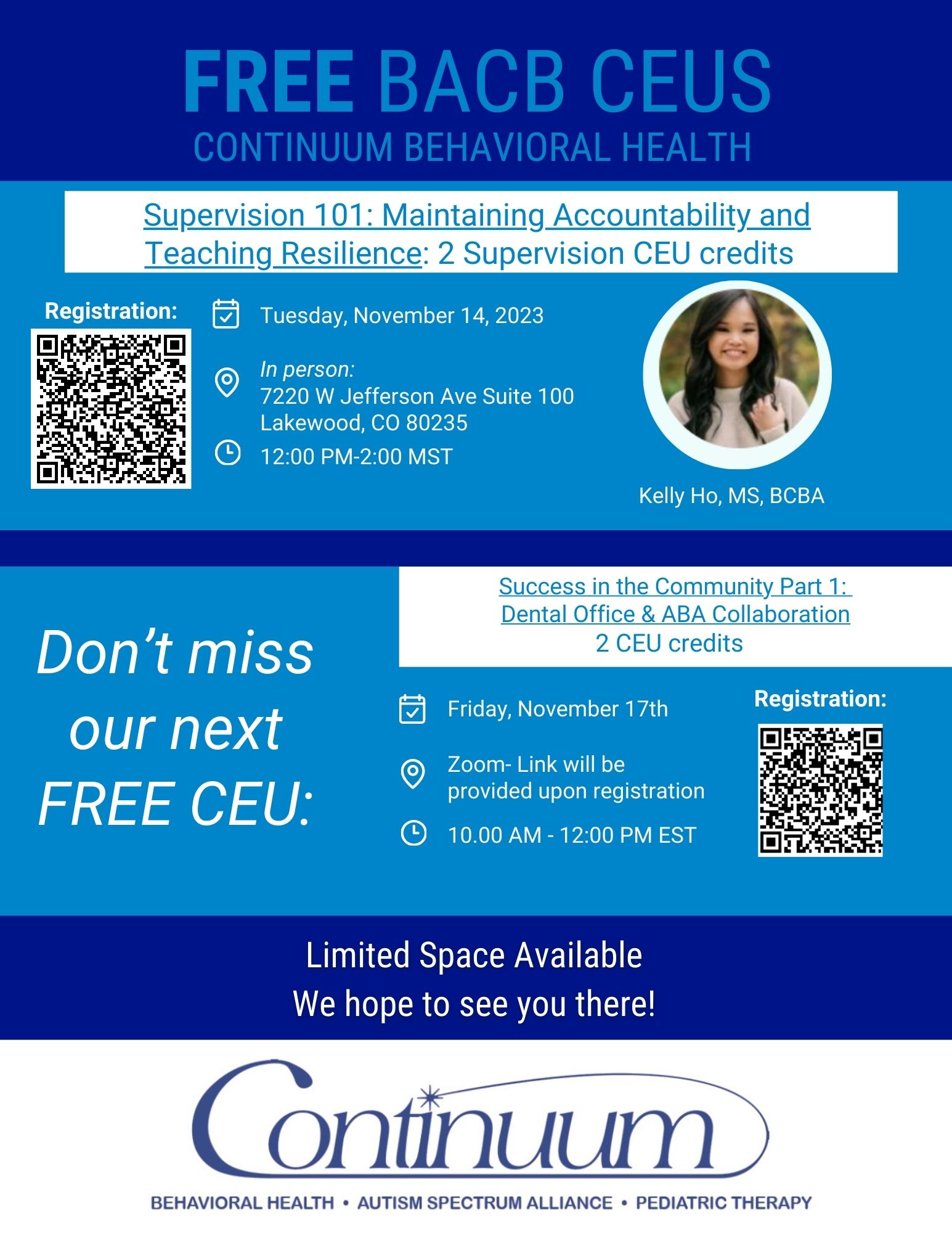
Dissemination
Increasing the awareness, knowledge, and utilization of existing methodologies and resources within our community
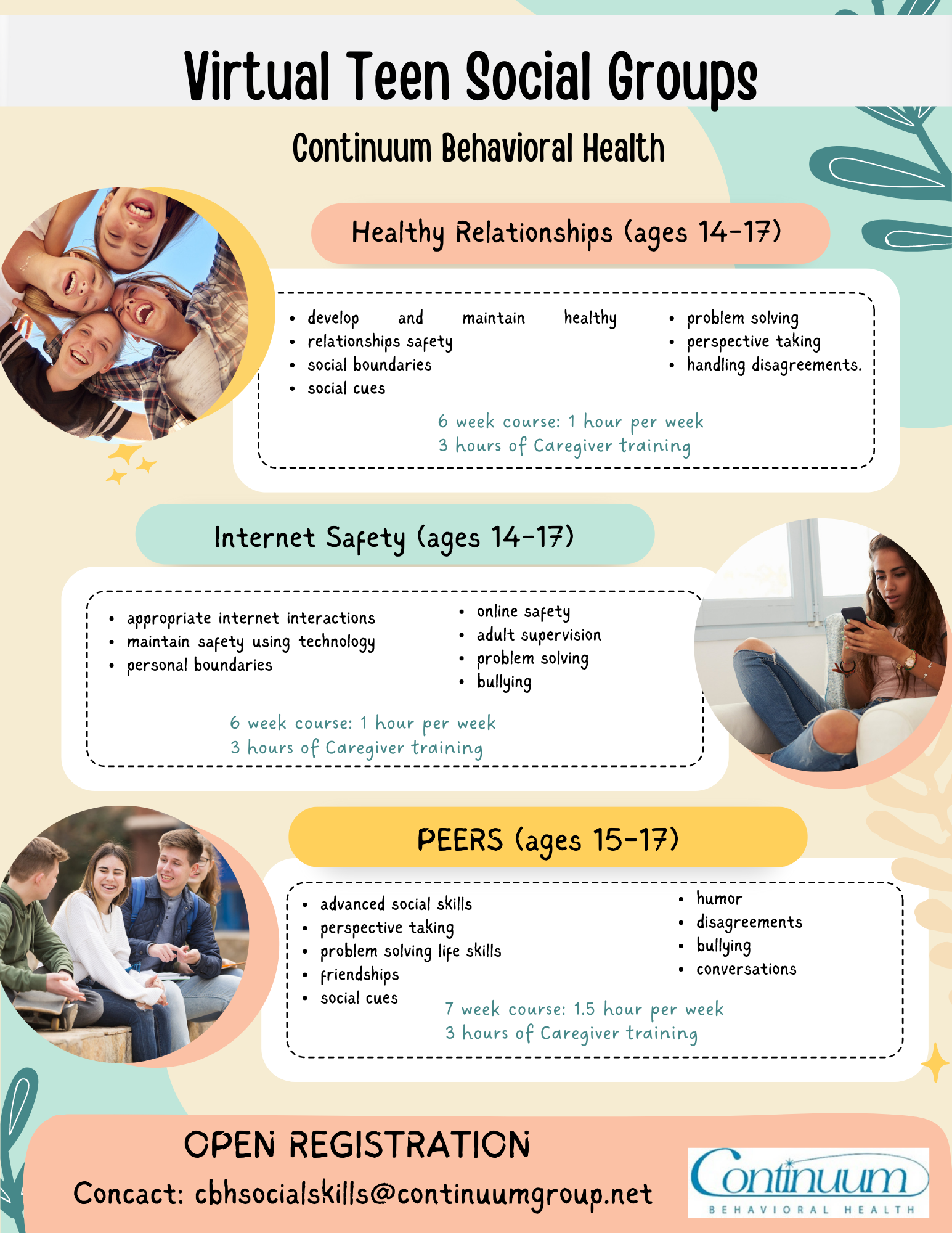
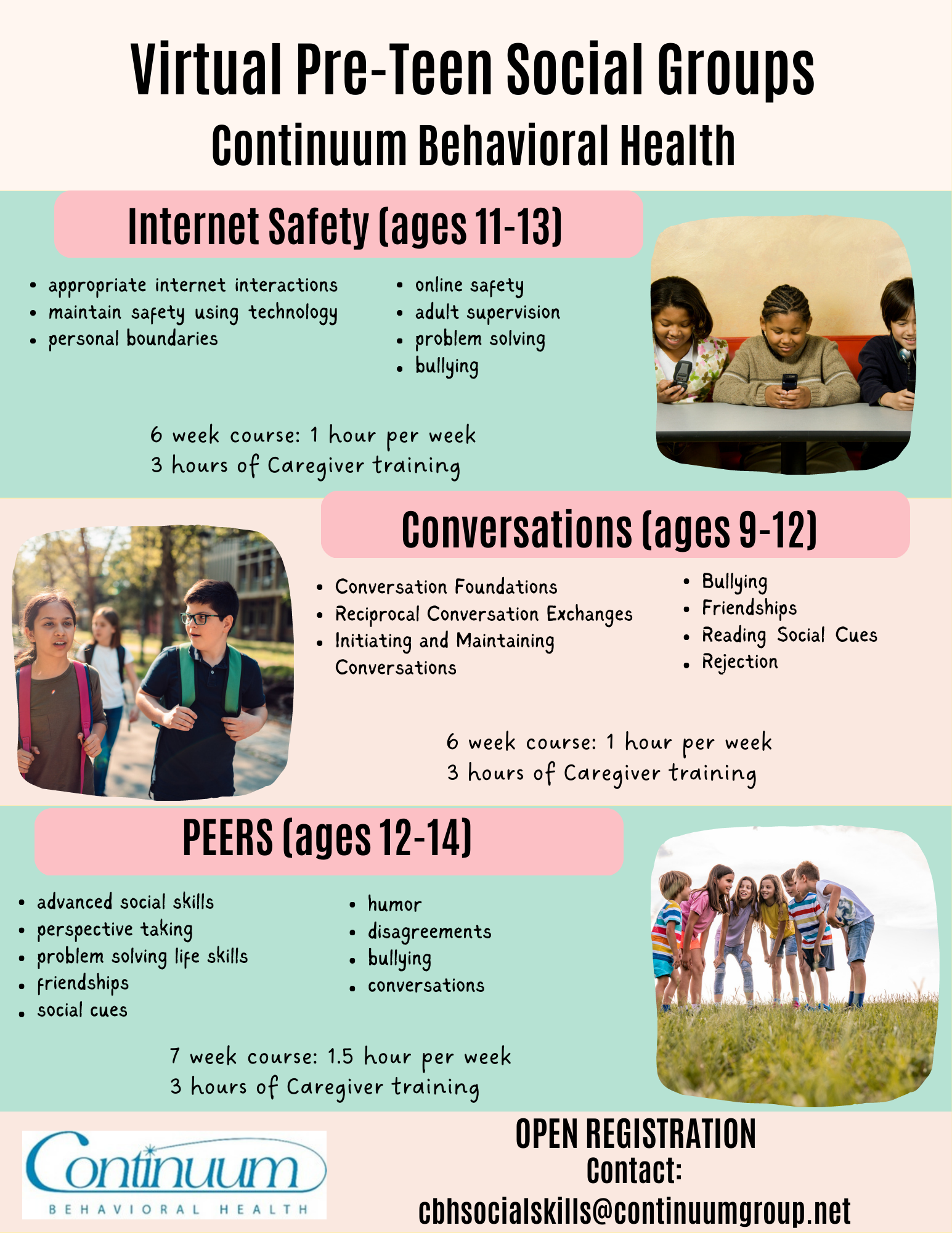
Clinical Services
At Continuum, we approach our services from a family-centered, client-focused lens that prioritizes a trusting relationship. Our goal is to help our clients and families reach their full potential and achieve their highest quality of life. We strive to achieve this goal by working collaboratively to ensure that treatment is focused on teaching meaningful goals and fostering social participation within the community.
Looking for a rewarding career where you will be impacting the quality of others? Looking for a fun and engaging work environment that offers employment flexibility and opportunities for growth? Then complete our application by clicking the APPLY NOW button!